Web-site restrictions
ACAT will be moving to a new web site on Thursday, 10th April.
In preparation, from Friday, 4th April this old web site will not let members renew their membership, and any other changes members make, e.g. their personal details, will get ‘lost in the move’.
Urgent membership renewals should instead be done by contacting Alison Marfell.
The States Description Procedure
Hubbuck, J., 2008. The States Description Procedure. Reformulation, Summer, pp.46-53.
Some Clinical Implications for the CAT Self-States Sequential Diagram [SSSD]
Introduction
Dr Anthony Ryle recently published his findings on the use of the States Description Procedure (SDP) questionnaires by patients with borderline personality disorder (BPD) (Ryle, 2007). I have recently extended my initial contribution to his sample from 9 to 35 BPD patients. He kindly provided me with regular email supervision on the SDP method, plus sometimes on clinical method. I now propose to publish my SDP results in the same journal (Hubbuck, 2008).
In this article I provide some brief results from my SDP sample and some brief comments on the new SCP format, as outlined by Ryle (2007) in the last issue of Reformulation. In the Appendix, I provide two case examples using a draft SCP pro-forma reporting format. Hopefully, this will aid CAT therapists in speedier production of SCP analyses for their patients. Finally, I explore what effect the SDP has had (and the SCP will have) for me in doing CAT maps (i.e. SSSDs).
Some Results from my SDP Sample
Currently, three of my new patients (2 males, 1 female) are scheduled to complete the SDP questionnaires soon. So I provide some brief conclusions from the 32 patients who have already completed the SDP. The relevant tables are shown, in summary form, below.
Table 1 shows male and female patients to be of similar mean age (total sample mean age about 34 years). Since these are private patients at the Priory Hospital (Marchwood, Southampton), mostly with medical insurance, they will tend to differ from BPD patients in the NHS. But they are unlikely to differ much in terms of severity of illness. Ryle’s Personality Structure Questionnaire (PSQ) (Pollock, et. al., 2001) total sample mean score (35.2), at the start of therapy, is very high on ‘borderline’ poorly controlled state switching. Ryle’s Severity Index (Ryle and Golynkina, 2000) mean (6.4) indicates that these patients’ lives are being seriously disrupted by their DSM-IV listed diagnostic criteria (American Psychiatric Association, 1994). The Beck Depression Inventory (BDI) (Beck et. al., 1968) overall mean score (30.9) indicates severe depression. The Burns Anxiety Inventory (BAI) (Burns, 1999) total mean score (48.2) indicates severe anxiety states. The Clinical Outcomes in Routine Evaluation (CORE) (Mental Health Foundation and CORE System Group, 200?) total score (71.9, mean 2.11) shows this to be much higher than the CORE User Manual clinical population mean of 1.86 and non-clinical mean of 0.76. Therefore, overall, at the start of CAT therapy, this BPD sample population has severe problems in terms of general social-psychological functioning and serious risk of self-harm. Males and females also have similar numbers of SDP-named states of mind (overall mean 8.2 states). Over one-third of these patients have been in-patients at the Priory Hospital, where I work, and also had CBT group therapy treatments. Out of 32 patients, four did not complete their CAT therapy (12.5%).
Table 2 shows the number and percentage of the sample that identified SDP-named states of mind as applying to themselves. This table also shows how often patients experienced these named states: either daily/weekly, or monthly/occasionally. Table 3 then puts these SDP-named states in rank order of incidence and compares this with the rank order of similar states identified by these patients in their CAT Psychotherapy File. States named in this File do not refer to frequency. So SDP-named and File-named comparative rankings are made mostly according to overall daily/weekly/ monthly frequency. Some of the File-named states are often not so precisely demarcated as distinct states of mind, when compared with the SDP-named states. However, the File-named states are often crucial components of well-constructed Self-States Sequential Diagrams (SSSDs).
Obviously, the CAT File provides a longer list of named states of mind than the SDP does. But the SDP provides more detailed information for each named state (in its shorter list). Therefore, the question arises: Why didn’t the SDP provide at least the same number of named states as the CAT File, if not more? This is a very complicated question to answer. It is outside the scope of this short article. Potentially, it could take us into deep questions like: Does every waking minute of a person’s conscious life have an underlying, nameable (emotional) state of mind? Or, are there times in cognitive thought processes that are not connected to nameable emotional states? Maybe I will risk getting into some of these complications in my later article (Hubbuck, 2008).
In the meantime Table 3 provides an opportunity to discuss whether or not the SDP-named and File-named rank orders for experiencing these states of mind point towards possible key states in BPD. However, this is only a rough and ready comparison. Clearly, it is not in any way psychometric.
Just highlighting some very brief comparisons: SDP-named and ranked states (1) ‘Soldiering-On’, (2) ‘Zombie-like’, (3) ‘Self-Critic’, and (4) ‘Rage’ also have broadly similar ranked numbers in the CAT File, i.e. (1), (3), (4) and (6) respectively. Only SDP-named and ranked (5=) ‘Victim-Abused’ state (i.e. = means an equal recorded incidence with ‘OK’ state) seems to relate to a range of six File-named states, i.e. (5=) ‘Misunderstood, Rejected, Abandoned’ and (7=) ‘Vulnerable, Needy, Helpless’ (waiting for rescue), (7=) ‘Clinging, Fearing Abandonment’, (8=) ‘Cheated by Life, by Others’ (untrusting), (8=) ‘Hurt, Humiliated by Others’, (12=) ‘Frightened of Others’. SDP-named (5=) ‘OK’ state drops to position (8), if SDP-named states are all ranked on daily/ weekly frequency only. This ‘OK’ state does not have a closely ranked equivalent from the CAT File. SDP-ranked (6) ‘High’, (7) ‘Obsessed-Compelled’ and (8=) ‘Powerful Caretaker’ perhaps sometimes relate to File-ranked (8=) ‘Frenetically Active’ (too busy to think or feel) and maybe to (11) ‘Resentfully Submitting to Others Demands.’ SDP-ranked (8=) ‘Dismissive-Contemptuous’ also compares closely with File-ranked (10) ‘Contemptuously Dismissive of Self’. Maybe SDP-named (9) ‘Revengeful’ and File-named (13) ‘Envious, Wanting to Harm Others’ bears some relationship, as does SDP (10) ‘Bully’ and CAT File (8=) ‘Hurting Self, Hurting Others’. SDP (11) ‘Cloud Cuckoo Land’ also perhaps relates to File-named (18) ranked state (not shown in Table 3), ie. ‘Feeling Perfectly Cared For, Blissfully Close to Another’.
Admittedly, this simple rank order comparison leaves much still open for debate and clarification. It seems to me that to decide on what are the most important, possibly pathological, states in BPD, then we need to try to answer the difficult question I outlined above. In other words, a major effort needs to be made to see if a named, underlying (emotional) state of mind can be identified for any period of time throughout the daily conscious life of any selected person. But of course there is the sensible need to have started somewhere practical. So I tend to agree with Ryle when he stated the following, in his recent article on the SDP:
“These (SDP) findings support the Multiple Self-States Model (MSSM) understanding of BPD as a consequence of childhood neglect and abuse leading to the internalisation of a negative main reciprocal role pattern. Patients re-enact and experience versions of that pattern in the Victim, Rage, Revengeful, Bully and Dismissive Contempt states. Much of the time, however, the experience or threat of abuse or abandonment, the sense of powerlessness or the fear of primitive, uncontrolled rage leads to dissociation. As was the case in childhood, this allows an escape from feared emotions, the dissociative process having become entrenched in the form of a repertoire of alternative states. These states may involve denial of the sense of weakness, as in the High state, or fantasised emotional safety, as in the Cloud Cuckoo Land, or the suppression of emotion, as in the Zombie state, or a combination of resentful submission and emotional flattening, as in the Soldiering On state. In the absence of threat some patients can experience the OK state or may guard against abandonment or abuse by caring for weak others in the Powerful Caretaker state.” (Ryle, 2007)
In my forthcoming article I hope to be able to show that, generally in BPD, there are perhaps two main negative reciprocal role patterns. Briefly, these can be characterised as mostly taking place in an ‘Ideal Care/ Perfect Attachment Trap’ and in a ‘Depressed Thinking/ Social Avoidance Trap’. So, given this SDP-based, Psychotherapy File-based and other sessional-based information, it is then up to the patient and therapist to collaborate in deciding how much key states of mind information finds its way onto the SSSD and where on the map it is all located. While my CAT maps err on the side of comprehensiveness they do tend, subject to individual variations, to include all of the states listed in Table 3. But maybe there are still some important states not listed in the SDP and the CAT File?
Some Thoughts on the SCP and on Further Research
Given that the SDP-named ‘Self-Critic’ rank is (3) and its File-named rank is (4) then ‘Self-Critic’ (guilty, blaming self, rejecting or hating self) seems to need a place in the list of common states in the SCP. In the case of patients with addiction presenting problems, it may be necessary to ask them to add ‘Addicted’ state (out of control, dangerously habitual, unable to stop) in the M, N, or O positions on the SCP list. But ‘Agitated, Confused, Anxious’, even though it ranks (2) in the Psychotherapy File, maybe does not need to be added to the SCP list. Like ‘Depressed’ state, it can be taken as a highly common state and both can be taken for granted as nearly always appearing on CAT maps. In the SCP ‘Frequency of State’ section, maybe it would be better if the old SDP format was reverted to. Perhaps further testing of the new SCP will throw up suggestions for change in some categories in C. ‘How you are in relation to yourself’. Therefore, I presume Ryle is likely to be requesting further testing of the SCP with patients before finalising the SCP. Currently, I am working on trying to draft a ‘States of Mind Inventory’ that could perhaps provide pre-therapy and post-therapy clinical scores.
Conclusions
Table 4 confirms that the SDP method is acceptable to patients. It shows that 29 patients (90.6%) thought that either the SDP was “of value”, or of “considerable value” to their therapy. This method helps change the way BPD patients think about their states of mind. To some extent it changed the way I think about them and the way I think about SSSDs. Writing many SDP reports for these patients led to an increased facility in explaining such states to them, as we engaged in the mapping process. I feel that this has enabled patients to accept and understand that it is best not to discount, or leave out, any key states of mind data. However, I always check carefully with my patients that their completed CAT map is not seen by them as too complex. Since very few say that it is, I am satisfied to err towards complexity, so that their social-psychological map does not lose any known significant states of mind data. Needless to say, these SSSDs still remain quite basic in relation to the complex operations of the human mind.
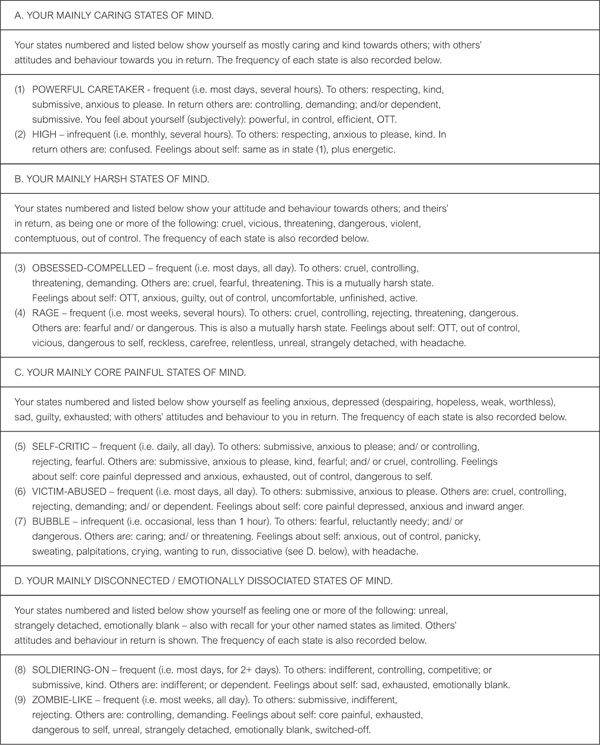
Siegel (1999) and some other psychiatrists argue that states of mind are probably the central organising function of the human mind (brain), interacting with our body systems and our social systems. This is consistent with CAT theory on ‘reciprocal role procedure’ (RRP-based) state switching as always involving “self to others”, “others to self”, and “self to self” (mind-body) interactions. As a result of the SDP reports written for them, the patients in this sample probably now see more clearly how their various named states are mainly harsh, caring, dissociative, core painful, or mixed states of mind. (See Appendix 1a). And as a result of our discussions about their SSSDs, most of these patients probably finished therapy viewing their states of mind as carriers of highly condensed, highly systemic, and highly important information about their life histories and life plans. Hopefully, I left them with the increased ability, in their everyday lives, to be able to ask themselves this regular question: “What named state of mind am I in at this moment; and what is the reason for it (in terms of my two emotional traps)?” This then adds to the likelihood of conscious, positive ‘traps exits’ being sought and not ‘autopilot’, negative ones.
So it would seem valuable to also test and report on the SCP, as the SDP has been tested. Hopefully, my proposed pro-forma reporting format (in Appendix 1) will help make quicker SCP analyses available to your patients. Maybe I will also be able to say more about the feasibility of a (longer) scored ‘States of Mind Inventory’ in my later article. That article will also provide clinical outcome scores at three month follow-up, for most of the patients in this sample. [Any comments please to: J.HUBBUCK@sky.com ]
References
Beck, A.T., Ward, C.H., Mendelson, M., Mock, J.E., and Erbaugh, J.K., (1968). An Inventory for Measuring Depression. Archives of General Psychiatry, 4, 561-571.
Burns, D. (1999). The Feeling Good Handbook: Revised Edition. Plume (Penguin Books). 43-44.
Clinical Outcomes in Routine Evaluation: CORE System User Manual (2006). Mental Health Foundation and CORE System Group.
Diagnostic and Statistical Manual of Mental Disorders. 301.83 Borderline Personality Disorder.
Disorders: Fourth Edition DSM-IV. (1994). American Psychiatric Association, Washington, DC. 650-654
Hubbuck, J. (2008). Clinical Psychology and Psychotherapy, (title and date of publication forthcoming).
Pollock, P., Broadbent, M., Clarke, S., Dorrian, A.J., and Ryle, A. (2001). The Personality Structure Questionnaire (PSQ): A measure of the multiple self-states model of identity disturbance in Cognitive Analytic Therapy. Clinical Psychology and Psychotherapy, 8, 59-72.
Ryle, A. (2007). Investigating the Phenomenology of Borderline Personality Disorder with the States Description Procedure: Clinical Implications. Clinical Psychology and Psychotherapy, 14, 5, 329-341.
Ryle, A. (2007a). States Characterisation Procedure (SCP): For supporting the reformulation of patients with borderline/ dissociative features (October 2007). Reformulation: Theory and Practice in CAT, 29, 9-11.
Ryle, A. and Golynkina, K. (2000). Effectiveness of time-limited Cognitive Analytic Therapy for borderline personality disorder: Factors associated with outcome. British Journal of Medical Psychology, 73, 197-210.
Siegel, D.J. (1999). The Developing Mind: How Relationships and the Brain Interact to Shape Who We Are. New York, The Guilford Press.

Table 1: Sex, Mean Age, Mean Initial Clinical Scores
and Mean Number of SDP-named States Identified for All Patients (n=32)
Clinical evaluation scores derived from Ryle’s Personality Structure Questionnaire (PSQ), Beck Depression Inventory (BDI), Burns Anxiety Inventory (BAI), the Clinical Outcomes in Routine Evaluation questionnaire (CORE), Ryle’s Severity Index (SI).
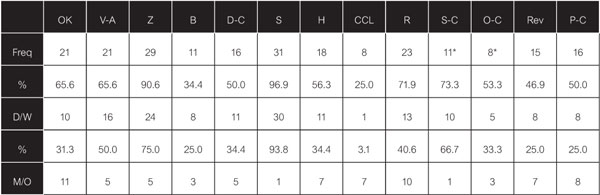
Table 2: SDP-Named States Identified by Number and Percentage of Patients,
Plus Frequency of Experiencing (ie. Daily/Weekly and Monthly/Occasionally (n=32)
State names: OK = OK-Normal, V-A = Victim-Abused, Z = Zombie-like, B = Bully, D-C = Dismissive-Contemptuous, S = Soldiering-On, H = High, CCL = Cloud Cuckoo Land, R = Rage, S-C = Self-Critic, O-C = Obsessed-Compelled, Rev. = Revengeful, P-C = Powerful Caretaker.
*Self-Critic and Obsessed-Compelled states were added to the SDP list of named states later on in this research. 15 patients were offered the choice of these two states. Of these 11 identified the former and 8 the latter state (ie. 73.3% and 53.3% respectively).
Table 3: Rank Order of SDP-Named States Experienced and
CAT Psychotherapy File-Named States Experienced (n=32)

SDP-Named States Rank Order Psychotherapy File Rank Order*
1. Soldiering-On 1. Solidering-On (feeling bad)
2. Zombie-Like 2. Agitated, Confused, Anxious
3. Self Critic 3. Zombie-Like (disconnected from feelings and others)
4. Rage 4. Intensely Critical of Self
5. Victim-Abused 5. Misunderstood, Rejected, Abandoned
5. OK 6. Rage (out of control)
6. High 7. Vulnerable, Needy, Helpless (waiting for rescue)
7. Obsessed-Compelled 7. Clinging, Fearing Abandonment
8. Powerful Caretaker 8. Cheated by Life, by Others (untrusting)
8. Dismissive Contemptuous 8. Frenetically Active (too busy to think or feel)
9. Revengeful 8. Hurting Self, Hurting Others.
10. Bully 9. Hurt, Humiliated by Others
11. Cloud Cuckoo Land 10. Contemptuously Dismissive of Self
11. Resentfully Submitting to Others’ Demands
12 Provoking, Teasing, Seducing (winding others up)
12. Frightened of Others
13. Envious, Wanting to Harm Others
* Data derived from “Different States of Mind” section of the CAT Psychotherapy File.
Table 4: Patients and Therapist Reporting Whether or Not the SDP Was of Value to the Therapy (n=32)

Of No Value Of Value Of Considerable Value
Patient 3 (9.4%) 13 (40.6%) 16 (50.0%)
Therapist 2 (6.2%) 10 (31.3%) 20 (62.5%)
Afterword
The development of the SDP and the derived SCP have been published; see references above. A great deal of this has been built on the systematic work of Jim Hubbuck, which he plans to continue. I hope there will be further extensions of the use of this approach and believe that anyone interested in participating in this should contact him. Anthony Ryle, May 2008.
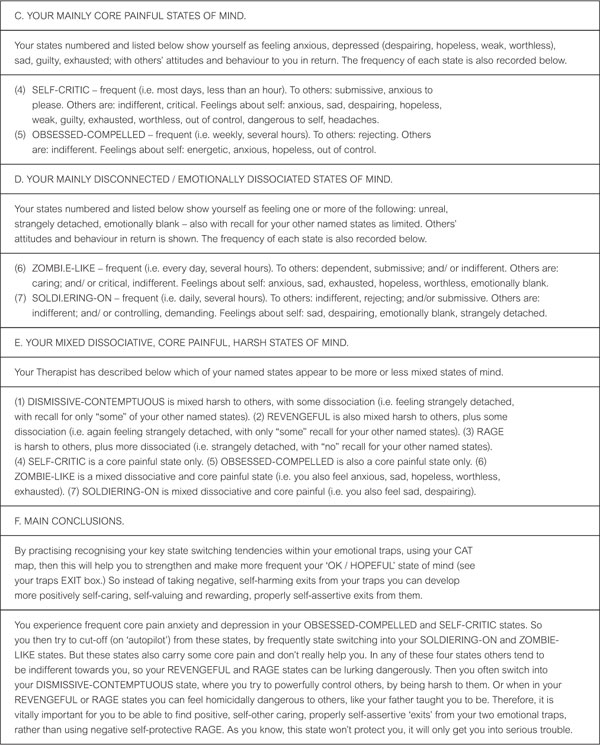
Appendix 1a
States Characterisation Procedure (SCP) Report For Your CAT Therapy: 9 Named States (Case 1 – Female)
Appendix 1a.
States Characterisation Procedure (SCP) Report For Your CAT Therapy: 7 Named States (Case 2 – Male)
Appendix 1b
Notes for CAT Therapists on Writing States Characterisation Procedure (SCP) Reports for Their Patients
Two examples of SCP reports are provided for your guidance in Appendix 1a. These case examples are based on SDP questionnaire results, but the report format is also appropriate for the new SCP questionnaires. This preferred report format arose out of detailed discussions with Dr Tony Ryle and detailed testing of alternative formats. With practise you can expect to produce similar reports in about an average time of 1 hour 15 minutes per report. These reports have been mostly “of considerable value” to patients (see Table 4 above).
Around session four, when you have a reasonable grasp of the patient’s life history and of their key social relationships, then seems to be the best time to ask them to fill in the SCP questionnaires. These results can then be incorporated into the developing SSSD map.
Using the guide under each heading A to D, sort out all the named states in the completed SCP questionnaires into groups under each heading. Then number and list them under each heading, in order of frequency. The above pro-forma report format uses Microsoft Word XP (click on the ‘Table’ tool and create a one column, one row table format for each section heading and section text). These ‘tables’ will then expand to fit the variable amount of text you create per section. The above examples use Times New Roman (font size 9 for the guides under each section; and font size 11 for the analysis text, under each section).
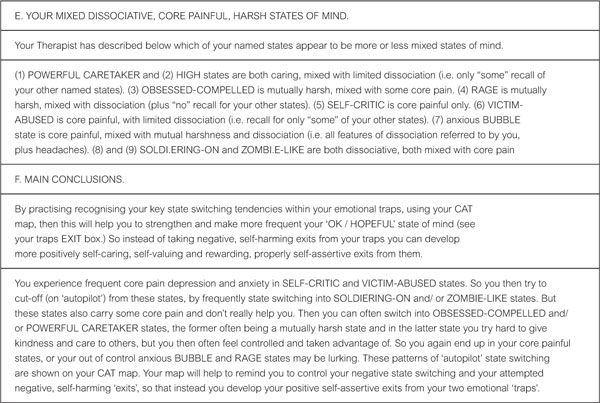
In sections A to D it is suggested that you stick with the categories for ordering of key adjectives (descriptors) of reciprocal role relationships, as in the above examples. These categories are: ‘To others’; ‘Others in return’; ‘Subjective feelings about self’. However, it is up to you as to how you highlight the 5 most important recorded adjectives (i.e. most typical, or most strong) under these three categories in A to D. Sections E and F are self-explanatory, using the headings guide.
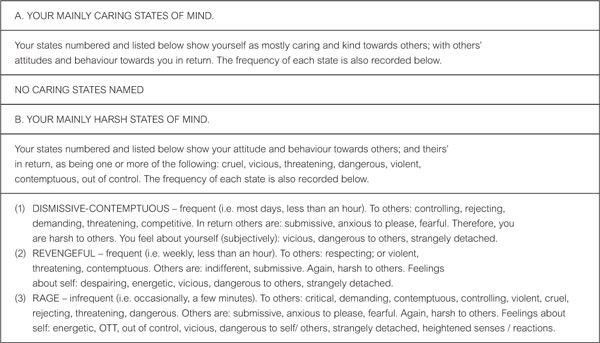
SCP case example 2 (male) said that his CAT map and his SCP (old SDP) report had helped him to see the “bigger picture” of his life and his “uncontrolled (autopilot) state switches within this bigger picture.” He also said that he could now see how he needs to fill the total gap in section A (i.e. ‘Mainly Caring States’) in his report, by developing a more self-caring and other-caring (‘OK/Hopeful’) state of mind, by “thinking inside my exits box on my map.” Conversely, in case example 1 (female) she said that she needed to reduce her frequent other-caring ‘Powerful Caretaker’ and less frequent ‘High’ states in section A, so as to develop a more frequent self-caring ‘OK/Hopeful’ state.
Full Reference
Hubbuck, J., 2008. The States Description Procedure. Reformulation, Summer, pp.46-53.Search the Bibliography
Type in your search terms. If you want to search for results that match ALL of your keywords you can list them with commas between them; e.g., "borderline,adolescent", which will bring back results that have BOTH keywords mentioned in the title or author data.
Related Articles
Draft States of Mind Inventory
Hubbuck, J., 2008. Draft States of Mind Inventory. Reformulation, Winter, pp.15-25.
States Characterisation Procedure (SCP) for supporting the reformulation of patients with borderline/dissociative features
Ryle, A., 2007. States Characterisation Procedure (SCP) for supporting the reformulation of patients with borderline/dissociative features. Reformulation, Winter, pp.9-11.
The States Description Procedure
Ryle, T., 2003. The States Description Procedure. Reformulation, Autumn, pp.13-16.
Letters to the Editors: Improve Your Reformulation and Contribute to Research - Try the States Description Procedure (SDP)
Ryle, T., 2003. Letters to the Editors: Improve Your Reformulation and Contribute to Research - Try the States Description Procedure (SDP). Reformulation, Spring, p.5.
The PSQ Italian Standardisation
Fiorani, C. and Poggioli, M., 2011. The PSQ Italian Standardisation. Reformulation, Winter, pp.49-52.
Other Articles in the Same Issue
CAT Used Therapeutically and Contextually
Murphy, N., 2008. CAT Used Therapeutically and Contextually. Reformulation, Summer, pp.26-30.
Catch up with CAT
Potter, S., Curran, A., 2008. Catch up with CAT. Reformulation, Summer, p.54.
Clinical Implications for the Pregnant CAT Therapist
Knight, A., 2008. Clinical Implications for the Pregnant CAT Therapist. Reformulation, Summer, pp.38-41.
Consent to Publish in Reformulation
Jenaway, A., Lloyd, J., 2008. Consent to Publish in Reformulation. Reformulation, Summer, p.7.
Cuckoo Lane
Selix, M., 2008. Cuckoo Lane. Reformulation, Summer, p.6.
How to Enjoy Writing a Prose Reformulation
Wilde McCormick, E., 2008. How to Enjoy Writing a Prose Reformulation. Reformulation, Summer, pp.16-17.
Integration of Cognitive Analytic Therapy Understandings
Ruppert, M., Birchnall, Z., Bruton, C., Christianson, S., 2008. Integration of Cognitive Analytic Therapy Understandings. Reformulation, Summer, pp.20-22.
Is CAT an Island or Solar System?
Bancroft, A., Collins, S., Crowley, V., Harding, C., Kim, Y., Lloyd, J., Murphy, N., 2008. Is CAT an Island or Solar System?. Reformulation, Summer, pp.23-25.
Letter from the Chair of ACAT
Westacott, M., 2008. Letter from the Chair of ACAT. Reformulation, Summer, pp.3-4.
Letter from the Editors
Elia, I., Jenaway, A., 2008. Letter from the Editors. Reformulation, Summer, p.3.
Metaprocedures in Normal Development and in Therapy
Hayward, M., McCurrie, C., 2008. Metaprocedures in Normal Development and in Therapy. Reformulation, Summer, pp.42-45.
Plugging in and Letting Go: the Use of Art in CAT
Hughes, R., 2008. Plugging in and Letting Go: the Use of Art in CAT. Reformulation, Summer, pp.9-10.
Service Innovation
Jenaway, A., Mortlock, D., 2008. Service Innovation. Reformulation, Summer, pp.31-32.
Silence in Practice
Harvey, L., 2008. Silence in Practice. Reformulation, Summer, pp.11-13.
The ‘Human Givens’ Fast Trauma and Phobia Cure
Jenaway, A., 2008. The ‘Human Givens’ Fast Trauma and Phobia Cure. Reformulation, Summer, pp.14-15.
The Body in Dialogue
Burns-Lundgren, E., Walker, M., 2008. The Body in Dialogue. Reformulation, Summer, pp.18-19.
The Development of the Sequential Diagrammatic Reformulation
Parkinson, R., 2008. The Development of the Sequential Diagrammatic Reformulation. Reformulation, Summer, pp.33-37.
The States Description Procedure
Hubbuck, J., 2008. The States Description Procedure. Reformulation, Summer, pp.46-53.
QuickLinks :: Members
QuickLinks :: Official
QuickLinks :: Practice
How does CAT work?
Key References about CAT
Regional Groups and SIGs
International CAT
Association for Cognitive Analytic Therapy Ltd
Company Registered In England 06063084
Registered Charity No 1141793
![]()
This site is designed and maintained by Alacrify